The impact of reflux disease on health-related quality of life and general wellbeing is often underplayed. However, this can be as bad or even worse as for someone suffering from medical conditions such as heart or lung disease.
The most common (typical) symptoms are
Less common (atypical) symptoms can include
Reflux symptoms can be very detrimental and may have a profound negative impact on health-related quality of life and general wellbeing. They interfere with work, sleep, leisure and relationships all of which makes life extremely miserable for sufferers. Other issues such as lethargy, fatigue and depressed mood can easily develop on the background of this chronic condition.
Poorly treated reflux can lead to significant and sometimes serious permanent damage to the oesophagus. These not only make symptoms even worse, but can develop into potentially life-threatening conditions including cancer.
Other medical conditions can arise or deteriorate secondary to reflux, including asthma, chest infections, anaemia and nutritional deficiencies.
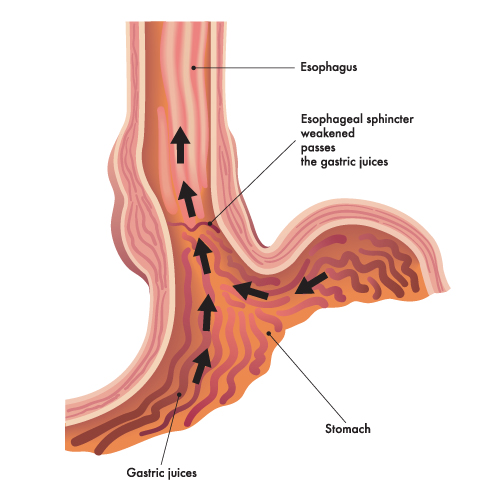
Gastro-oesophageal reflux usually occurs because of an ineffective valve between the oesophagus and stomach. However other problems may also be present which can give rise to very similar symptoms.
The oesophagus (gullet) is a hollow muscular tube-like organ which leads from the back of the mouth into the stomach. Its main purpose is to allow swallowed food and liquid (bolus) to safely pass from the back of the mouth (pharynx) into the stomach. This simple task does however require complex co-ordination of its muscles in a manner to propel the bolus – this is referred to as peristalsis.
In addition, two valves, which act as gates must open and close at exactly the right time, and with the right amounts of pressure.
The first valve is the upper oesophageal sphincter (UOS). This is normally tightly shut, which is very important as it prevents material from the digestive tract from entering the voice box (larynx) and breathing airways (trachea and bronchus).
As food leaves the pharynx, this valve very briefly opens at the exact same time as the entrance to the larynx is slammed shut, allowing the bolus to pass safely, and then immediately closes again as the entrance to the larynx is re-opened for normal breathing and talking.
This whole process takes a fraction of a second, and is a reflex (automatic co-ordination of the nerves and muscles) which we cannot consciously control.
Problems with this mechanism can give rise to many of the symptoms associated with GORD, but are in fact not due to this as the main problem. Some of these conditions are referred to as laryngo-pharyngeal-reflux (LPR).
After passing through the first valve, the bolus is then normally propelled along the length of the oesophagus, which is approximately 25cm long, by peristalsis.
Problems with the peristalsis mechanism, another automatic reflex, however can result in the bolus becoming stuck or delayed causing dysphagia and even to move back up the oesophagus as regurgitation. Conditions that are related to issue are referred to as oesophageal motility disorders, and result in symptoms again similar to GORD.
At the lower end of the oesophagus, the propulsion of the bolus stimulates another automatic reflex, this time causing the lower oesophageal sphincter (LOS), the second valve, to open.
Like the UOS, this is normally shut, and keeps the contents of the stomach in place. It can open and close, and this is important in being able to pass wind (burping) and when necessary vomit. Both these natural functions are automatic reflex controlled. During swallowing, it opens to allow the bolus to enter the stomach, and then closes again.
GORD occurs when the LOS cannot maintain an effective barrier between the stomach and oesophagus.
The stomach itself is a large bag-like organ where the process of digestion begins. It can become very full after large meals.
Enzymes and fluid, including acid are secreted by the cells in the lining of the stomach which starts to break down the food materials, allowing nutrients to be released. This may take several hours, after which the part-digested material is released into the duodenum, another tube-like organ for further digestion to occur.
Another valve (the pylorus) controls this passage, and problems with this valve can give rise to reflux from the duodenum, which is alkaline and contains bile to enter the stomach, and if the LOS is also defective, enter the oesophagus. This condition is referred to as duodeno-gastro-oesophageal-reflux (DGOR).
I wanted to say thank you for everything you have done for me by offering me the LINX Surgery and completely changing my quality of life for the better.
The oesophagus is exposed to excessive amounts of fluid from the stomach which contains acid, bile and enzymes. This corrosive chemical causes intense stimulation of the nerve fibres in the oesophagus which sends these signals to the brain. It is here where the symptoms are perceived in the same way as any other painful stimulus (e.g. pricking your finger or stubbing your toe), except in reflux you cannot see what is happening.
The relationship between the brain and gut is fascinating, but currently not very well understood. Some people are more sensitive than others (oesophageal hypersensitivity) and get very bad symptoms even with small amounts of reflux, whilst others, despite having significant levels of recorded reflux do not appear to have such bad problems even though their oesophagus is severely damaged.
The lining of the oesophagus reacts and becomes inflamed (oesophagitis) in reflux, which can lead to erosions, ulcers and scarring, which can be permanent. The cells lining the lower oesophagus, which are not normally resistant to this exposure can also change completely and become more like the cells lining the stomach. This is known as Barrett’s metaplasia and is associated with a risk of developing cancer.
Reflux often (but not always) occurs in conjunction with a hiatus hernia, where a portion of the upper stomach migrates into the chest.
Sometimes people have many of the symptoms of reflux, but no evidence of actual reflux or other associated conditions can be found. This is referred to as a functional disorder, and frequently such individuals also have problems throughout the whole of the gut. This is not surprising, as in fact the gut is one-long hollow muscular organ – the gastro-intestinal tract, with the oesophagus, stomach and duodenum just being at the start, or upper end.
Gastro-oesophageal reflux disease, or simply reflux, is a common condition afflicting millions of people in the UK.
Symptoms of reflux can be very serious and affect work, disrupt sleep, impair leisure activities and upset relationships, all of which lead to a profound negative impact on general health and wellbeing.
South West Reflux offer effective treatment options including novel LINX reflux management system as well as standard keyhole anti-reflux surgery. These aim to give sufferers of reflux freedom from symptoms and escape drug dependency.
You can call us on 01392 796880 or get in touch via our online contact form.
